Working Length in Endodontics: Why Apex Locators Usually Get It Right
May 24, 2026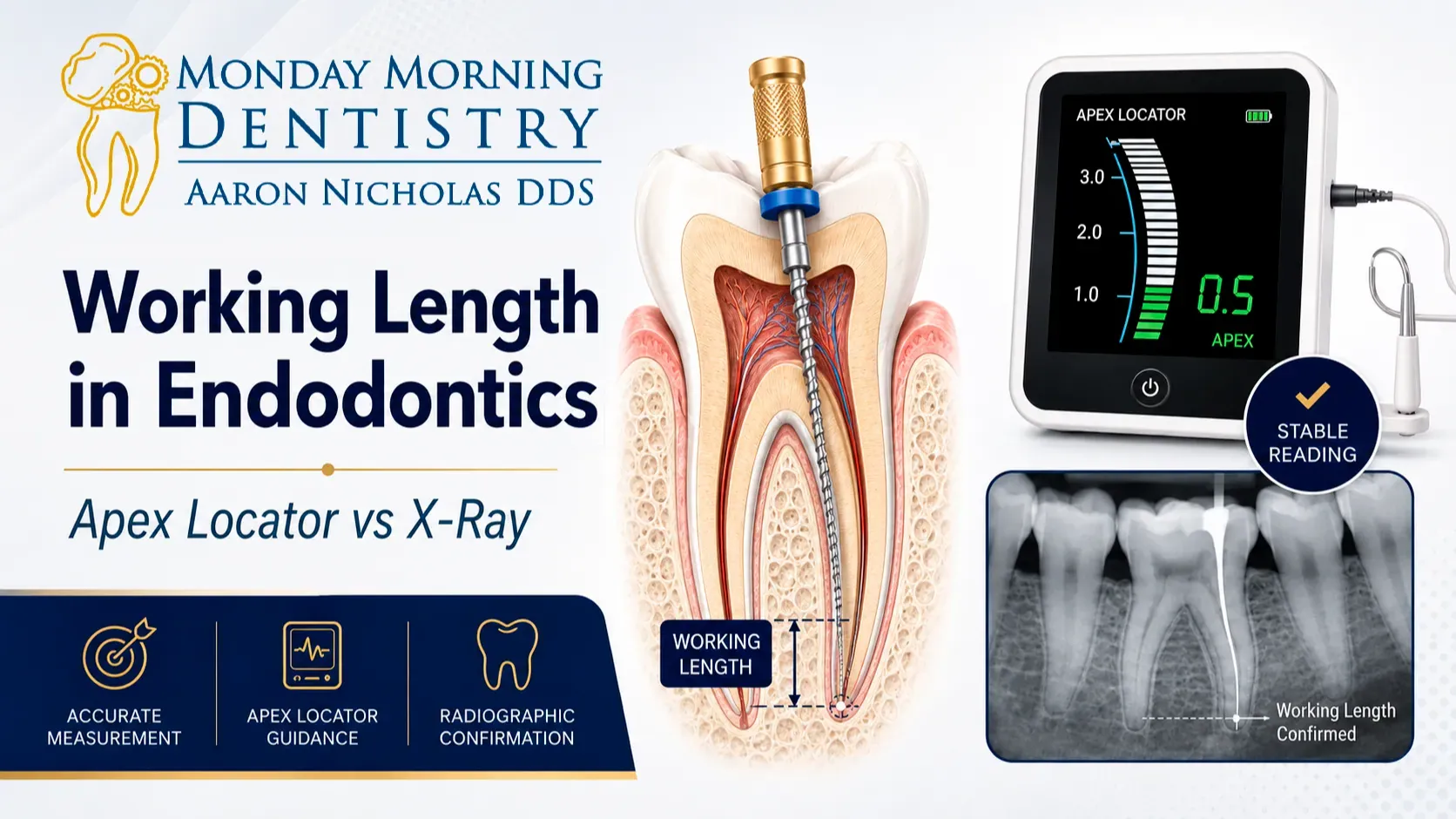
Most endodontic errors don't happen in the obturation. They happen earlier — quietly — when working length is off by a millimeter.
Instrument too short and you leave bacteria behind. Instrument too long and you've irritated the periapical tissues, set up post-op sensitivity, and handed yourself a problem you'll be explaining at the recall appointment. Every experienced clinician knows this. The hard part isn't understanding it. The hard part is getting it right when the schedule is full and the day is moving fast.
Why X-Rays Don't Give You the Whole Picture
Radiographic working length was the standard for decades. Measure to the radiographic apex. Subtract 1 mm. Confirm with a film. Move on.
It works — until it doesn't.
The problem is what that method assumes: that the end of the root on the x-ray corresponds to where the canal actually terminates internally. That's often not the case.
The apical constriction — the anatomic endpoint you're actually targeting — can sit short of the radiographic apex. It can exit laterally. It can behave in ways a 2D image simply won't reveal. That's not pathology. That's normal root canal anatomy.
So a case can look perfect on film and still heal unpredictably. The radiograph told you one story. The apex told a different one.
What an Apex Locator Actually Measures
An electronic apex locator doesn't work like a ruler. It detects changes in electrical impedance as the file moves toward the periapical tissues — giving you real-time feedback about where you actually are in the canal, not just where the canal looks like it ends on a flat image.
When apex locator readings are stable and conditions are right, they're remarkably consistent. The device isn't the weak link.
The setup is.
Root canal working length accuracy with an apex locator depends on:
- Complete isolation
- A clean pulp chamber before you start
- Proper irrigation throughout
- The correct file size and canal fit
- Management of infection, hemorrhage, and excess fluid
Skip any of those steps and the readings bounce. That's when dentists blame the apex locator. The apex locator didn't fail — the conditions did.
Use the tool correctly and it becomes one of the most reliable instruments in the procedure.
When the Readings Don't Settle
You've seen it. Numbers jumping around. Measurements that don't match what you expected. Readings that change every time — or don't move at all.
When that happens, don't guess. Don't average it out and hope for the best.
Unstable apex locator readings are almost always a signal, not a failure. They're pointing back to something earlier in the sequence:
- Pulp chamber not fully cleaned out
- File doesn't match the canal or isn't seated correctly
- Debris or fluid disrupting the circuit
- Canal not negotiated to the apex yet
Sometimes the right call is to temporize and schedule a second visit. Not every case should be finished in one appointment. Pushing through unstable conditions creates post-op problems and turns a manageable case into a difficult one.
Apex Locator vs Radiograph — Use Both
This is not an either/or. It never should have been.
The apex locator finds your working length. The radiograph confirms anatomy and gives you documentation. Together, they eliminate guesswork and make root canal working length more accurate than either tool could on its own.
{place image here: periapical radiographs — short, ideal, and long working length}
When they don't agree, that's information. It usually means something about the anatomy, the canal curvature, or the conditions during measurement. Don't ignore the discrepancy. Follow it.
Working Length on a Full Schedule
On a slow day, this step feels straightforward. On a full day, it can feel rushed — and rushed working length creates compounding problems.
If your working length feels inconsistent case to case, that's rarely a skill problem. It's almost always a system problem. The steps aren't being done in the same order every time. The setup isn't consistent. Pressure is filling in the gaps where process should be.
When chairside assistants are trained to set up the room completely, place the rubber dam correctly, and support the irrigation and file sequence, working length becomes predictable. Not because the doctor is trying harder — but because the conditions for accuracy are built into the workflow.
That's the difference between a good outcome and a consistent one.
The Monday Morning Dentistry Approach
At MMD, we focus on what actually works in real practices — not ideal-conditions dentistry.
Apex locators are a core part of that. When they're used with the right setup and taken seriously as a clinical step — not a shortcut — they make working length faster and more reliable.
That same logic runs through everything we teach: clear steps, a logical sequence, and decisions that hold up on a Monday morning when the schedule is full and there's no margin for error.
Apex locators work when the setup is right. Radiographs still matter — but as support, not replacement. Predictable endodontic outcomes start with a consistent sequence, and working length is one of the most important steps in that sequence. Get this right every time, and everything downstream gets easier.
